




LESSONS LEARNED IN THE DESIGN AND IMPLEMENTATION OF MODULAR HOSPITALS IN PERU
A technical approach based on the preparation of technical files, current health regulations, and post-COVID experience
03/03/2026
1. Executive Summary
Modular hospitals originated in Peru as an urgent response to a crisis that tested not only the healthcare system but also our capacity to care for people when they needed it most. Behind each module, each technical decision, and each solution improvised by the emergency, there was a common purpose: to protect and save human lives. This article compiles the lessons learned in the design and implementation of these infrastructures, reminding us that the planning, design, and management of a hospital are never abstract exercises but profoundly human endeavors, and that strengthening them is essential so that, in the face of any new emergency, the infrastructure is up to the task of safeguarding the lives it is meant to protect.
2. Introduction
The historical gap in hospital infrastructure in Peru[1], coupled with the pressure generated by the COVID-19 pandemic, spurred the accelerated adoption of unconventional solutions for the provision of health services. In this context, modular hospitals became established as a rapidly deployable alternative to increase installed capacity, especially in Category I and II health facilities, or in hybrid configurations between both categories.
This situation arose, in many cases, because facilities initially designed for lower complexity required the incorporation of Health Service Production Units (UPSS) typical of category II-1—such as the Obstetrics Center, the Surgical Center, and Hospitalization areas—in order to meet a demand for care that exceeded their original capacity. As a result, facilities were created whose categorization was not clearly defined, as they combined services from different levels of care within an infrastructure designed to be temporary.
Experience has shown that such temporary measures, initially conceived as a transitional condition, ultimately become ineffective in the face of a structural healthcare gap that necessitates the continued operation of infrastructure originally designed for emergencies. Thus, what was designed as a temporary solution ends up fulfilling permanent functions, without necessarily having been conceived for prolonged operation.
It should be noted that, from a regulatory standpoint, there is currently no specific regulation defining the minimum characteristics of a contingency hospital or a modular facility intended for temporary use. The available technical framework is primarily limited to the Technical Document entitled “Technical Criteria for Infrastructure and Equipment for the Design of Temporary Care Environments in Health Facilities,” approved by the Ministry of Health in 2023[2], which establishes infrastructure and equipment criteria for the design of temporary care environments in health facilities, without comprehensively addressing the functional, operational, and sustainability implications of these hospitals when their use is extended over time.
While the temporary nature of these healthcare facilities allowed for a timely response to a public health emergency, it also revealed significant technical, regulatory, and operational limitations when these infrastructures transitioned from temporary use to long-term operation. Many of the problems identified were not related to the modular system itself, but rather to deficiencies in planning, technical design, and the preparation of documentation, including technical specifications, technical files, and terms of reference for procurement.
A critical factor was the contracting method used in various hospital projects, where the implementation of modular hospitals was treated as the acquisition of goods rather than as a construction project. This directly impacted the level of technical, regulatory, and quality control required at each stage and for each deliverable. The absence of proper construction supervision, often replaced by limited technical assistance, significantly reduced the ability to control the correct implementation of the modules that comprised each Health Service Production Unit (UPSS).
This situation was exacerbated in facilities located in remote or difficult-to-access areas, where the frequency of technical visits was restricted by logistical factors, affecting the continuous verification of the execution, assembly, and compatibility of the engineering specialties. In the context of infrastructure designed as temporary, these deficiencies might have seemed minor; however, as operations extended over time, they became structural problems that impacted the functionality, safety, and sustainability of the facilities.
In this context, this article systematically develops the main lessons learned in the design and implementation of modular hospitals in Peru, integrating regulatory criteria from the Ministry of Health (MINSA), the National Building Regulations (RNE), and practical experience in the preparation of technical files, as well as in the technical monitoring and follow-up of this type of infrastructure.
3. Modular Contingency Hospitals: Concept and Problems
Modular contingency hospitals are health infrastructures made up of industrialized construction systems, prefabricated totally or partially off-site, which are assembled on the assigned land through assembly processes designed for accelerated implementation.
These systems can be based on three-dimensional container-type modules, industrialized structural panels, or hybrid solutions, depending on the supplier and the functional scope of the establishment.
From a regulatory standpoint, it is crucial to clarify that the modular nature of the project does not exempt it from compliance with current health and construction regulations. Modular hospitals must adhere to the Ministry of Health's (MINSA) Technical Health Standards, the design criteria for hospital infrastructure and equipment, and the applicable chapters of the National Building Regulations (RNE), particularly those related to safety and evacuation, electrical and plumbing installations, mechanical systems, and telecommunications systems. Furthermore—and equally important—the necessary pre-installations for the proper implementation of medical equipment must be provided.
However, in practice, the applicable regulations were not always fully implemented, citing the temporary nature of the infrastructure, which led to technical gaps that became apparent once healthcare operations began. This situation highlights a key lesson: Modularity is not a normative shortcut, but a constructive strategy that demands a higher level of technical anticipation and stricter coordination between disciplines.
«"Modularity is not a regulatory shortcut, but a constructive strategy that demands a higher level of technical anticipation and stricter coordination between disciplines."»
In the case of hospital infrastructure, this requirement is critical due to the high concentration of specialized facilities and the need for each of these systems—architecture, structure, installations, and equipment—to be properly integrated. Only through adequate technical integration is it possible to guarantee the optimal and safe operation of the healthcare facility throughout its lifespan, even when it was originally conceived as a contingency solution..
4. Planning and definition of the scope of care
One of the most recurring errors identified in modular hospitals is the lack of a clear definition of the facility's lifespan. Projects conceived as temporary were later incorporated into the permanent healthcare network, even though their structural, architectural, and installation designs had not been intended for continuous operation.
«"One of the most recurring errors identified in modular hospitals is the lack of a clear definition of the facility's useful life. Projects conceived as temporary were later incorporated into the permanent healthcare network, without their structural, architectural, or installation design having been intended for continuous operation."»
From the planning stage, it is essential to define the level of care, the service portfolio, and the functional requirements according to the facility's categorization, as per the regulations of the Ministry of Health (MINSA). Failure to do so leads to delayed redesigns that, in industrialized systems, have a significantly greater economic and technical impact than in traditional construction.
5. Lessons learned
To present the lessons learned in a structured manner, four representative models are developed below, organized by problem, recurring cause, impact on operations, and technical recommendation. These models do not aim to encompass all identified situations, but rather to highlight those with the highest recurrence and greatest impact on the sustainability of the establishments.
LESSON LEARNED 1: Gaps in the definition of scope in contracting documents
In the case of modular contingency hospitals, one of the most recurring problems arises from the very definition of the project scope. Frequently, this scope is limited to a nominal statement—the project title—without precisely detailing the size of the temporary hospital, the services it includes, and those that are expressly excluded.
Defining the scope involves clearly establishing, from the planning stage, the criteria that determine which Health Service Production Units (HSPUs) will be implemented, their level of complexity, how they will be interconnected, and under what assumptions regarding demand, growth, and operation. This must be complemented by an explicit definition of the temporary nature of the establishment, understanding that this condition not only corresponds to an operational timeframe but also to technical decisions consistent with a limited lifespan.
In this sense, a hospital designed as temporary should not incorporate systems and facilities intended for long-term operation, such as oversized solutions, permanent networks without dismantling criteria, or configurations that hinder future adaptation or removal. The lack of this distinction has, in practice, led to hybrid infrastructures: facilities designed with temporary needs in mind, but partially equipped as permanent hospitals, without either approach being fully integrated.
«"The lack of this differentiation has, in practice, generated hybrid infrastructures: establishments designed with criteria of temporaryity, but partially equipped as permanent hospitals, without either approach having been developed in an integrated way."»
All these criteria must be clearly described and formalized in the terms of reference, technical specifications, or tender documents for the implementation of modular hospitals. A poorly defined scope in these contractual documents not only weakens the technical control of the project but also negatively impacts the quality of the design, the compatibility of specialties, and ultimately, the functionality and sustainability of the facility during its operation.
The following matrix exemplifies one of the most recurring lessons learned in the implementation and contractual formulation of modular hospital projects: the insufficient formulation of the Terms of Reference as the starting point of the project.
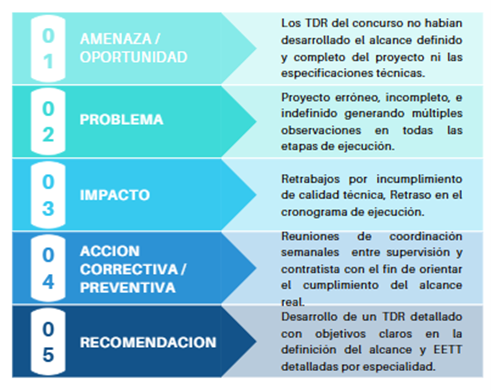
The diagram above identifies the initial threat as the lack of a fully developed scope and technical specifications in the tender's Terms of Reference. This results in an incomplete and undefined project, subject to numerous observations during its execution. This deficiency generates rework, technical non-compliance, and schedule delays. Experience demonstrates that the quality of design and execution depends largely on the clarity and precision with which the scope and specifications are defined from the contracting stage.
LESSON LEARNED 2: Defining the technical team as a guarantee of project quality
A second recurring lesson identified in the implementation of modular hospitals relates to defining the required technical team in the contract documents. Experience shows that the quality of the design and execution depends not only on the clarity of the scope, but also on the profile, specialization, and experience of the key personnel responsible for the project's development.
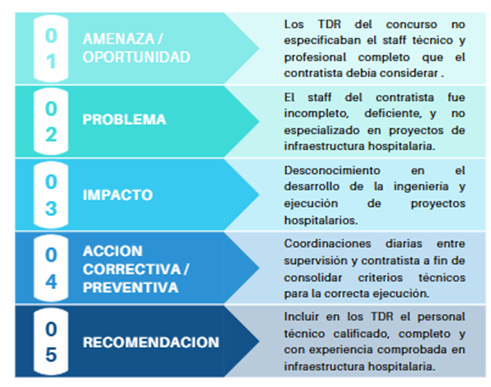
The presented scheme demonstrates that the lack of a precise definition of key technical staff in the Terms of Reference results in incomplete teams or teams with insufficient experience in hospital infrastructure, directly impacting the quality of the engineering work and the proper execution of the project. In the hospital setting, where multiple technical specialties and critical systems converge, the lack of professionals with specialized experience increases the risk of compatibility errors, facility deficiencies, and inadequate technical decisions.
The lesson learned is clear: the requirement for a qualified, complete technical team with proven experience in health infrastructure must be established from the contract formulation stage, as it is a determining factor to ensure the sustainability and proper functioning of the hospital establishment.
LESSON LEARNED 3: Quality management as a cross-cutting pillar in modular hospital projects
A third lesson identified in the implementation of modular hospitals relates to the contractor's organizational management and quality systems. In hospital projects, where technical, environmental, and occupational safety requirements converge, management capacity is as crucial as the technical capacity for design or execution.

The diagram shows that the contractor's lack of policies, internal regulations, management manuals, and formal quality systems leads to deficiencies in the overall management of the project. The absence of a robust management structure directly impacts project delays, environmental risks, inadequate occupational safety conditions, and a decline in technical quality. While the supervisor is authorized to implement corrective controls to mitigate these deficiencies, experience demonstrates that management cannot rely solely on reactive measures.
The lesson learned is this: contracting documents must require from the outset the presentation and validation of quality, environmental management and occupational health and safety plans, recognizing that hospital infrastructure demands organizational standards equivalent to its technical complexity.
LESSON LEARNED 4: Early management of procedures and basic services as a critical factor in the schedule
A fourth lesson learned from the implementation of modular hospitals relates to managing procedures with providers of basic services, such as electricity, water, and sewage. In many projects, these procedures were not considered an integral part of the contractual timeline, leading to delays that directly impacted the opening of the hospital.
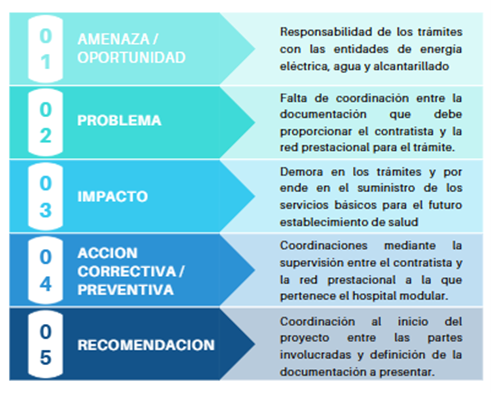
The diagram shows that the lack of a clear definition of responsibility for procedures and coordination between the contractor and the service provider network leads to delays in obtaining essential basic services for the operation of the healthcare facility. In hospital projects, where the physical infrastructure cannot function without electricity, potable water, and functioning sanitation systems, the timely management of these procedures is as critical as the architectural design or the internal installations.
The observed case studies confirm that early coordination between the parties involved and the precise definition of the required documentation must be incorporated from the beginning of the project to prevent administrative factors from becoming technical and operational risks.
The four models presented constitute a representative sample of the most recurring lessons learned in the implementation of modular contingency hospitals. They do not encompass all situations identified throughout the accumulated experience; rather, they reveal structural patterns that are repeated at different stages of the project cycle: formulation of the contractual scope, definition of the technical team, organizational management, and inter-institutional coordination. Systematizing these lessons learned allows us to understand that the main risks do not originate in the modular construction system itself, but rather in the planning, integration, and control processes that surround it.
The massive implementation of modular hospitals during the COVID-19 pandemic yielded specific lessons for the Peruvian context. Many of these facilities were conceived and built under emergency criteria, with extremely tight deadlines and technical decisions dictated by the urgency, which severely limited the comprehensive planning processes required for a healthcare facility.
In this context, the experience gained from the technical review and monitoring of modular hospitals implemented during the health emergency revealed that the lack of sufficiently developed technical documentation transfers significant technical risks to the operational phase. These deficiencies subsequently manifested as higher maintenance costs, unforeseen adaptation needs, and difficulties in ensuring optimal operating conditions once the critical phase of the pandemic had passed.
In light of this experience, the lessons learned acquire strategic value. Their systematization and incorporation as institutional roadmaps is fundamental to avoiding the repetition of errors associated with a lack of planning, particularly in a country that is not immune to facing new health emergencies. Likewise, these lessons should guide the future development of contingency hospitals as part of a progressive strategy to reduce, as much as possible, the hospital infrastructure gap that still persists in Peru.
«"Given this experience, the lessons learned acquire strategic value. Their systematization and incorporation as institutional roadmaps is fundamental to avoiding the repetition of errors associated with a lack of planning, particularly in a country that is not exempt from facing new health emergencies."»
6. Conclusions
Modular hospitals represent a viable solution for expanding hospital capacity, provided they are approached with the same technical rigor as conventional infrastructure. The Peruvian experience demonstrates that the main problems identified do not stem from the modular system itself, but rather from deficiencies in the design, the definition of the scope, and the preparation of the technical documentation that supported its implementation.
The experience gained in preparing and reviewing technical files for Category I and II modular hospitals confirms that systematizing lessons learned is a key tool for continuous improvement. The use of lesson-learning matrices by stage and specialty, technical feedback mechanisms, and regulatory checklists directly contributes to reducing recurring errors and raising the technical quality of projects.
Integrating early on the regulations of the Ministry of Health (MINSA), the National Building Regulations (RNE) and the lessons learned from the post-COVID period allows adapting solutions conceived in emergency contexts into safe, functional and sustainable infrastructures, aligned with the real needs of the health system and with a life cycle vision.
It is equally important to acknowledge that the technical evaluation of various modular hospitals implemented during the emergency demonstrated that, when properly designed and managed, they achieved functional and operational levels that, in certain contexts, surpassed those of existing conventional facilities. This achievement was made possible by the commitment and responsibility of technical teams and public officials who, in a context of high uncertainty, opted for alternative solutions to address a critical healthcare need.
Recovering and valuing this experience, from a technical and objective perspective, is a collective responsibility. Strengthening planning, learning from mistakes, and building on successes will allow the country to face future health emergencies with greater preparedness, without losing sight of the fact that the ultimate goal of all hospital infrastructure is to protect and save lives.
[1] See Diagnosis of infrastructure or access gaps to services in the Health Sector (2027-2029), prepared within the framework of General Directive of the National System of Multiannual Programming and Investment Management, approved by Directive No. 001-2019-EF/63.011, August 2025.
[2] Ministerial Resolution No. 468-2023-MINSA, issued on May 18, 2023, approved the Technical Document: "Technical Criteria for Infrastructure and Equipment for the Design of Temporary Care Environments in Health Establishments.".

Mg. Architect Daphne Olga Narciso Maldonado
Chapter 5989
Specialist in Architecture, Signage, Safety and Evacuation
Expert consultantta CLG
«"Modularity is not a regulatory shortcut, but a constructive strategy that demands a higher level of technical anticipation and stricter coordination between disciplines."»
«"One of the most recurring errors identified in modular hospitals is the lack of a clear definition of the facility's useful life. Projects conceived as temporary were later incorporated into the permanent healthcare network, without their structural, architectural, or installation design having been intended for continuous operation."»
«"The lack of this differentiation has, in practice, generated hybrid infrastructures: establishments designed with criteria of temporaryity, but partially equipped as permanent hospitals, without either approach having been developed in an integrated way."»
«"Given this experience, the lessons learned acquire strategic value. Their systematization and incorporation as institutional roadmaps is fundamental to avoiding the repetition of errors associated with a lack of planning, particularly in a country that is not exempt from facing new health emergencies."»
